Vitamin K
Vitamin K (K from "Koagulations-Vitamin" in German and Scandinavian languages[1]) denotes a group of lipophilic, hydrophobic vitamins that are needed for the posttranslational modification of certain proteins, mostly required for blood coagulation, but also a number of other proteins that chelate calcium ions and are involved in bone and other tissue metabolism. They are 2-methyl-1,4-naphthoquinone derivatives.
Vitamin K1 is also known as phylloquinone or phytomenadione (also called phytonadione). Vitamin K2 (menaquinone, menatetrenone) is normally produced by bacteria in the large intestine,[2] and dietary deficiency is extremely rare unless the intestines are heavily damaged, are unable to absorb the molecule, or are subject to decreased production by normal flora, as seen in broad spectrum antibiotic use.[3]
There are three synthetic forms of vitamin K, vitamins K3, K4, and K5, which are used in many areas including the pet food industry (vitamin K3) and to inhibit fungal growth (vitamin K5).[4]
Chemical structure
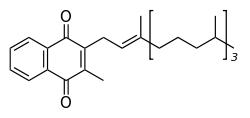
All members of the vitamin K group of vitamins share a methylated naphthoquinone ring structure, and vary in the aliphatic side chain attached at the 3-position (see figure 1). Phylloquinone (also known as vitamin K1) invariably contains in its side chain four isoprenoid residues, one of which is unsaturated.
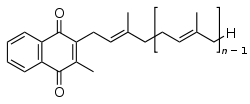
Menaquinones have side chains composed of a variable number of unsaturated isoprenoid residues; generally they are designated as MK-n, where n specifies the number of isoprenoids.
It is generally accepted that the naphthoquinone is the functional group, so that the mechanism of action is similar for all K-vitamins. Substantial differences may be expected, however, with respect to intestinal absorption, transport, tissue distribution, and bio-availability. These differences are caused by the different lipophilicity of the various side chains, and by the different food matrices in which they occur.
Physiology
Vitamin K is involved in the carboxylation of certain glutamate residues in proteins to form gamma-carboxyglutamate residues (abbreviated Gla-residues). The modified residues are often (but not always) situated within specific protein domains called Gla domains. Gla-residues are usually involved in binding calcium. The Gla-residues are essential for the biological activity of all known Gla-proteins.[5]
At this time[update] 14 human proteins with Gla domains have been discovered, and they play key roles in the regulation of three physiological processes:
- Blood coagulation: (prothrombin (factor II), factors VII, IX, X, protein C, protein S, and protein Z).[6]
- Bone metabolism: osteocalcin, also called bone Gla-protein (BGP), and matrix gla protein (MGP).[7]
- Vascular biology.[8]
Like other liposoluble vitamins (A, D, E), vitamin K is stored in the fat tissue of the human body.
Recommended amounts
The U.S. Dietary Reference Intake (DRI) for an Adequate Intake (AI) of vitamin K for a 25-year old male is 120 micrograms/day. The Adequate Intake (AI) for adult women is 90 micrograms/day, for infants is 10–20 micrograms/day, for children and adolescents 15–100 micrograms/day. In 2002 it was found that to get maximum carboxylation of osteocalcin, one may have to take up to 1000 μg of vitamin K1.[9]
Toxicity
Although allergic reaction from supplementation is possible, there is no known toxicity associated with high doses of the phylloquinone (vitamin K1) or menaquinone (vitamin K2) forms of vitamin K and therefore no tolerable upper intake level (UL) has been set.
However, a synthetic form of vitamin K, vitamin K3 (menadione), is demonstrably toxic. In fact, the FDA has banned this synthetic form of the vitamin from over-the-counter supplements because large doses have been shown to cause allergic reactions, hemolytic anemia, and cytotoxicity in liver cells.[10]
Drug Interactions
Phylloquinone (K1)[11][12] or menaquinone (K2) are capable of blocking the blood thinning action of anticoagulants like warfarin, which work by interfering with the action of vitamin K. They also reverse the tendency of these drugs to cause arterial calcification in the long term.
Sources
Vitamin K1 is found chiefly in leafy green vegetables such as spinach, swiss chard, and Brassica (e.g. cabbage, kale, cauliflower, broccoli, and brussels sprouts); some fruits such as avocado and kiwifruit are also high in vitamin K. By way of reference, two tablespoons of parsley contain 153% of the recommended daily amount of vitamin K.[13] Some vegetable oils, notably soybean, contain vitamin K, but at levels that would require relatively large caloric consumption to meet the USDA recommended levels.[14]
It is believed that phylloquinone's tight binding to the thylakoid membranes in the chloroplasts is the reason behind the poor bioavailability of vitamin K in green plants. For example, cooked spinach has a 5 percent bioavailability of phylloquinone. However when one adds fat to the spinach, the bioavailability increases to 13 percent due to the increased solubility of vitamin K in fat.[15]
Menaquinone-4 and menaquinone-7 (vitamin K2) are found in meat, eggs, dairy,[16] and natto[17]. MK-4 is synthesized by animal tissues, the rest (mainly MK-7) are synthesized by bacteria during fermentation. In natto 0% of vitamin K is from MK-4 and in cheese 2–7%.[18]
Deficiency
Average diets are usually not lacking in vitamin K and primary vitamin K deficiency is rare in healthy adults. As previously mentioned, newborn infants are at an increased risk of deficiency. Other populations with an increased prevalence of vitamin K deficiency include individuals who suffer from liver damage or disease (e.g. alcoholics), people with cystic fibrosis, inflammatory bowel diseases or those who have recently had abdominal surgeries. Groups that may suffer from secondary vitamin K deficiency include bulimics, those on stringent diets, and those taking anticoagulants. Other drugs that have been associated with vitamin K deficiency include salicylates, barbiturates, and cefamandole, although the mechanism is still unknown. There is no difference between the sexes as both males and females are affected equally. Symptoms of deficiency include heavy menstrual bleeding in women, anemia, bruising, and bleeding of the gums or nose. They could also have disorders such as coagulopathy.[18]
Osteoporosis[19][20] and coronary heart disease[21][22] are strongly associated with lower levels of K2 (menaquinone). Menaquinone is not inhibited by salicylates as happens with K1, so menaquinone supplementation can alleviate the chronic vitamin K deficiency caused by long term aspirin use.
Biochemistry
Discovery
In 1929, Danish scientist Henrik Dam investigated the role of cholesterol by feeding chickens a cholesterol-depleted diet.[23] After several weeks, the animals developed hemorrhages and started bleeding. These defects could not be restored by adding purified cholesterol to the diet. It appeared that—together with the cholesterol—a second compound had been extracted from the food, and this compound was called the coagulation vitamin. The new vitamin received the letter K because the initial discoveries were reported in a German journal, in which it was designated as Koagulationsvitamin. Edward Adelbert Doisy of Saint Louis University did much of the research that led to the discovery of the structure and chemical nature of vitamin K.[24] Dam and Doisy shared the 1943 Nobel Prize for medicine for their work on vitamin K (K1 and K2) published in 1939. Several laboratories synthesized the compound(s) in 1939.[25]
For several decades the vitamin K-deficient chick model was the only method of quantifying vitamin K in various foods: the chicks were made vitamin K-deficient and subsequently fed with known amounts of vitamin K-containing food. The extent to which blood coagulation was restored by the diet was taken as a measure for its vitamin K content. Three groups of physicians independently found this: Biochemical Institute, University of Copenhagen (Dam and Johannes Glavind), University of Iowa Department of Pathology (Emory Warner, Kenneth Brinkhous, and Harry Pratt Smith), and the Mayo Clinic (Hugh Butt, Albert Snell, and Arnold Osterberg).[26]
The first published report of successful treatment with vitamin K of life-threatening hemorrhage in a jaundiced patient with prothrombin deficiency was made in 1938 by Smith, Warner, and Brinkhous.[27]
Function
The function of vitamin K in the cell is to convert glutamate in proteins to gamma-carboxyglutamate (gla).
Within the cell, vitamin K undergoes electron reduction to a reduced form of vitamin K (called vitamin K hydroquinone) by the enzyme vitamin K epoxide reductase (or VKOR).[28] Another enzyme then oxidizes vitamin K hydroquinone to allow carboxylation of Glu to Gla; this enzyme is called the gamma-glutamyl carboxylase[29][30] or the vitamin K-dependent carboxylase. The carboxylation reaction will only proceed if the carboxylase enzyme is able to oxidize vitamin K hydroquinone to vitamin K epoxide at the same time; the carboxylation and epoxidation reactions are said to be coupled reactions. Vitamin K epoxide is then re-converted to vitamin K by vitamin K epoxide reductase. These two enzymes comprise the so-called vitamin K cycle.[31] One of the reasons humans are rarely deficient in vitamin K is that vitamin K is continually recycled in our cells.
Warfarin and other coumarin drugs block the action of the vitamin K epoxide reductase.[32] This results in decreased concentrations of vitamin K and vitamin K hydroquinone in the tissues, such that the carboxylation reaction catalyzed by the glutamyl carboxylase is inefficient. This results in the production of clotting factors with inadequate Gla. Without Gla on the amino termini of these factors, they no longer bind stably to the blood vessel endothelium and cannot activate clotting to allow formation of a clot during tissue injury. As it is impossible to predict what dose of warfarin will give the desired degree of suppression of the clotting, warfarin treatment must be carefully monitored to avoid over-dosing. (See the warfarin article.)
Gamma-carboxyglutamate proteins, or Gla-proteins
At present, the following human Gla-containing proteins have been characterized to the level of primary structure: the blood coagulation factors II (prothrombin), VII, IX, and X, the anticoagulant proteins C and S, and the Factor X-targeting protein Z. The bone Gla-protein osteocalcin, the calcification inhibiting matrix gla protein (MGP), the cell growth regulating growth arrest specific gene 6 protein (Gas6), and the four transmembrane Gla proteins (TMGPs) the function of which is at present unknown. Gas6 can function as a growth factor that activates the Axl receptor tyrosine kinase and stimulates cell proliferation or prevents apoptosis in some cells. In all cases in which their function was known, the presence of the Gla-residues in these proteins turned out to be essential for functional activity.
Gla-proteins are known to occur in a wide variety of vertebrates: mammals, birds, reptiles, and fish. The venom of a number of Australian snakes acts by activating the human blood clotting system. Remarkably, in some cases activation is accomplished by snake Gla-containing enzymes that bind to the endothelium of human blood vessels and catalyze the conversion of procoagulant clotting factors into activated ones, leading to unwanted and potentially deadly clotting.
Another interesting class of invertebrate Gla-containing proteins is synthesized by the fish-hunting snail Conus geographus.[33] These snails produce a venom containing hundreds of neuro-active peptides, or conotoxins, which is sufficiently toxic to kill an adult human. Several of the conotoxins contain 2–5 Gla residues.[34]
Methods of assessment
Prothrombin time test:
- Measures the time required for blood to clot
- Blood sample mixed with citric acid and put in a fibrometer.
- Delayed clot formation indicates a deficiency.
Unfortunately insensitive to mild deficiency as the values do not change until the concentration of prothrombin in the blood has declined by at least 50 percent [35]
Plasma Phylloquinone:
- Was found to be positively correlated with phylloquinone intake in elderly British women, but not men [36]
However an article by Schurges et al. reported no correlation between FFQ and plasma phylloquinone [37]
Urinary γ-carboxyglutamic acid:
- Urinary Gla responds to changes in dietary vitamin K intake.
- Several days are required before any change can be observed.
In a study by Booth et al. increases of phylloquinone intakes from 100 μg to between 377–417 μg for 5 days did not induce a significant change Response may be age-specific [38]
Function in bacteria
Many bacteria, such as Escherichia coli found in the large intestine, can synthesize vitamin K2 (menaquinone),[39] but not vitamin K1 (phylloquinone). In these bacteria, menaquinone will transfer two electrons between two different small molecules, in a process called anaerobic respiration.[40] For example, a small molecule with an excess of electrons (also called an electron donor) such as lactate, formate, or NADH, with the help of an enzyme, will pass two electrons to a menaquinone. The menaquinone, with the help of another enzyme, will in turn transfer these 2 electrons to a suitable oxidant, such fumarate or nitrate (also called an electron acceptor). Adding two electrons to fumarate or nitrate will convert the molecule to succinate or nitrite + water, respectively. Some of these reactions generate a cellular energy source, ATP, in a manner similar to eukaryotic cell aerobic respiration, except that the final electron acceptor is not molecular oxygen, but say fumarate or nitrate (In aerobic respiration, the final oxidant is molecular oxygen (O2) , which accepts four electrons from an electron donor such as NADH to be converted to water.) Escherichia coli can carry out aerobic respiration and menaquninone-mediated anaerobic respiration.
Vitamin K injection in newborns
The blood clotting factors of newborn babies are roughly 30 to 60 percent that of adult values; this may be due to the reduced synthesis of precursor proteins and the sterility of their guts. Human milk contains between 1 and 4 micrograms/litre of vitamin K1, while formula derived milk can contain up to 100 micrograms/litre in supplemented formulas. Vitamin K2 concentrations in human milk appear to be much lower than those of vitamin K1. It is estimated that there is a 0.25 to 1.7 percent occurrence of vitamin K deficiency bleeding in the first week of the infant's life with a prevalence of 2-10 cases per 100,000 births.[41] Premature babies have even lower levels of the vitamin and are at a higher risk from this deficiency.
USA
As a result of the occurrences of vitamin K deficiency bleeding, the Committee on Nutrition of the American Academy of Pediatrics has recommended that 0.5 to 1.0 mg vitamin K1 be administered to all newborns shortly after birth.[42]
UK
In the UK, vitamin K is administered to newborns as either a single injection at birth or three orally administered doses given at birth and then over the baby's first month.
Controversy
Controversy arose in the early 1990s regarding this practice when two studies were shown suggesting a relationship between parenteral administration of vitamin K and childhood cancer (14). However, poor methods and small sample sizes led to the discrediting of these studies and a review of the evidence published in 2000 by Ross and Davies found no link between the two.[43]
Dietary Vitamin K and bone health
There is physiological and observational evidence that Vitamin K plays a role in bone growth and the maintenance of bone density, but efforts to delay the onset of osteoporosis by Vitamin K supplementation have proven ineffective.
Biophysical studies have indicated that supplemental vitamin K promotes osteotrophic processes and slows osteoclastic processes via calcium bonding. Other studies have shown that vitamin K antagonists (usually a class of anticoagulants) lead to early calcification of the epiphysis and epiphysial line in mice and other animals, causing seriously decreased bone growth. This is due to defects in osteocalcin and matrix gla protein. Their primary function is to prevent overcalcification of the bone and cartilage. Vitamin K is important in the process of carboxylating glutamic acid (Glu) in these proteins to gamma-carboxyglutamic acid (Gla), which is necessary for their function.[44][45]
Data from the 1998 Nurses Health Study, an observational study, indicated an inverse relationship between dietary vitamin K1 and the risk of hip fracture. After being given 110 micrograms/day of vitamin K, women who consumed lettuce one or more times per day had a significantly lower risk of hip fracture than women who consumed lettuce one or fewer times per week. In addition to this, high intakes of vitamin D but low intakes of vitamin K were suggested to pose an increased risk of hip fracture.[46] [45]
However, a large multicentre randomized placebo-controlled trial was performed to test the supplementation of Vitamin K in post-menopausal women with osteopenia. Despite heavy doses of Vitamin K, no differences were found in bone density between the supplemented and placebo groups.[47]
In Japan, a form of vitamin K2 is recognized as a treatment for osteoporosis.[48][46] However the long term effects and benefits are unknown and it remains controversial.
Vitamin K and Alzheimer's disease
Research into the antioxidant properties of vitamin K indicates that the concentration of vitamin K is lower in the circulation of carriers of the APOE4 gene, and recent studies have shown its ability to inhibit nerve cell death due to oxidative stress. It has been hypothesized that vitamin K may reduce neuronal damage and that supplementation may hold benefits to treating Alzheimer's disease, although more research is necessary in this area.[49]
Vitamin K used topically
Vitamin K may be applied topically, typically as a 5% cream, to diminish postoperative bruising from cosmetic surgery and injections, broken capillaries (spider veins), to treat rosacea and to aid in the fading of hyperpigmentation and dark under-eye circles.
Vitamin K and cancer
While researchers in Japan were studying the role of vitamin K2 in the prevention of bone loss in females with liver disease, they discovered another possible effect of this phytonutrient. This two year study which involved 21 women with viral liver cirrhosis found that women in the supplement group were 90 percent less likely to develop liver cancer.[50][51] A German study performed on men with prostate cancer found a significant inverse relationship between vitamin K2 consumption and advanced prostate cancer.[52]
Vitamin K as antidote for poisoning by 4-hydroxcoumarin drugs
Vitamin K is a true antidote for poisoning by 4-hydroxycoumarin anticoagulant drugs (sometimes loosely referred to a coumarins). These include the pharmaceutical warfarin, and also anticoagulant-mechanism poisons such as bromadiolone, which are commonly found in rodenticides. 4-hydroxycoumarin drugs possess anticoagulatory and rodenticidal properties because they can completely block synthesis of vitamin K in the liver. Death is usually a result of internal hemorrhage. Treatment usually consists of repeated intravenous doses of vitamin K, followed by doses in pill form for a period of at least two weeks, though possibly up to 2 months, afterwards (in the case of the more potent 4-hydoxycoumarins used as rodenticides). If caught early, prognosis is good, even when great amounts of the drug or poison are ingested.
History of discovery
The precise function of vitamin K was not discovered until 1974, when three laboratories (Stenflo et al.[53], Nelsestuen et al.[54], and Magnusson et al.[55]) isolated the vitamin K-dependent coagulation factor prothrombin (Factor II) from cows that received a high dose of a vitamin K antagonist, warfarin. It was shown that while warfarin-treated cows had a form of prothrombin that contained 10 glutamate amino acid residues near the amino terminus of this protein, the normal (untreated) cows contained 10 unusual residues that were chemically identified as gamma-carboxyglutamate, or Gla. The extra carboxyl group in Gla made clear that vitamin K plays a role in a carboxylation reaction during which Glu is converted into Gla.
The biochemistry of how vitamin K is used to convert Glu to Gla has been elucidated over the past thirty years in academic laboratories throughout the world.
References
- ↑ Dam, Henrik (1935). "The antihaemorrhagic vitamin of the chick". The Biochemical journal 29 (6): 1273–85. PMID 16745789. PMC 1266625. http://www.biochemj.org/bj/029/1273/0291273.pdf.
- ↑ Bowen, R. "Large Intestine". Colostate. http://www.vivo.colostate.edu/hbooks/pathphys/misc_topics/vitamink.html. Retrieved 2009-06-01.
- ↑ "Vitamin K". http://www.nlm.nih.gov/medlineplus/druginfo/natural/patient-vitamink.html. Retrieved 2009-05-26.
- ↑ McGee, W (2007-02-01). "Vitamin K". MedlinePlus. http://www.nlm.nih.gov/medlineplus/ency/article/002407.htm. Retrieved 2009-04-02.
- ↑ Furie B, Bouchard BA, Furie BC (15 March 1999). "Vitamin K-dependent biosynthesis of gamma-carboxyglutamic acid". Blood 93 (6): 1798–808. PMID 10068650. http://bloodjournal.hematologylibrary.org/cgi/content/full/93/6/1798.
- ↑ Mann KG (1999). "Biochemistry and physiology of blood coagulation". Thromb. Haemost. 82 (2): 165–74. PMID 10605701. http://www.schattauer.de/index.php?id=1268&pii=th99080165&no_cache=1.
- ↑ Price PA (1988). "Role of vitamin-K-dependent proteins in bone metabolism". Annu. Rev. Nutr. 8: 565–83. doi:10.1146/annurev.nu.08.070188.003025. PMID 3060178.
- ↑ Berkner KL, Runge KW (2004). "The physiology of vitamin K nutriture and vitamin K-dependent protein function in atherosclerosis". J. Thromb. Haemost. 2 (12): 2118–32. doi:10.1111/j.1538-7836.2004.00968.x. PMID 15613016. http://www.blackwell-synergy.com/doi/full/10.1111/j.1538-7836.2004.00968.x.
- ↑ Neil C Binkley, Diane C Krueger, Tisha N Kawahara, Jean A Engelke, Richard J Chappell and John W Suttie. "A high phylloquinone intake is required to achieve maximal osteocalcin {gamma}-carboxylation". American Journal of Clinical Nutrition 76 (5).
- ↑ Higdon (February 2008). "Vitamin K". Linus Pauling Institute, Oregon State University. http://lpi.oregonstate.edu/infocenter/vitamins/vitaminK/. Retrieved 2008-04-12.
- ↑ Ansell J, Hirsh J, Poller L, Bussey H, Jacobson A, Hylek E (2004). "The pharmacology and management of the vitamin K antagonists: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy". Chest 126 (3 Suppl): 204S–233S. doi:10.1378/chest.126.3_suppl.204S. PMID 15383473. http://www.chestjournal.org/cgi/content/full/126/3_suppl/204S. (summary)
- ↑ Crowther MA, Douketis JD, Schnurr T, et al. (2002). "Oral vitamin K lowers the international normalized ratio more rapidly than subcutaneous vitamin K in the treatment of warfarin-associated coagulopathy. A randomized, controlled trial" (PDF). Ann. Intern. Med. 137 (4): 251–4. PMID 12186515. http://www.annals.org/cgi/reprint/137/4/251.
- ↑ Nutrition Facts and Information for Parsley, raw
- ↑ Nutrition facts, calories in food, labels, nutritional information and analysis – NutritionData.com
- ↑ NutritionData.com
- ↑ Elder SJ, Haytowitz DB, Howe J, Peterson JW, Booth SL (January 2006). "Vitamin k contents of meat, dairy, and fast food in the u.s. Diet". J. Agric. Food Chem. 54 (2): 463–7. doi:10.1021/jf052400h. PMID 16417305.
- ↑ Tsukamoto Y, Ichise H, Kakuda H, Yamaguchi M (2000). "Intake of fermented soybean (natto) increases circulating vitamin K2 (menaquinone-7) and gamma-carboxylated osteocalcin concentration in normal individuals". J. Bone Miner. Metab. 18 (4): 216–22. doi:10.1007/s007740070023. PMID 10874601. http://link.springer.de/link/service/journals/00774/bibs/0018004/00180216.htm.
- ↑ 18.0 18.1 "On the Trail of the Elusive X-Factor: Vitamin K2 Revealed". http://westonaprice.org/basicnutrition/vitamin-k2.html#fig4.
- ↑ Ikeda; Iki, M; Morita, A; Kajita, E; Kagamimori, S; Kagawa, Y; Yoneshima, H (2006). "Intake of fermented soybeans, natto, is associated with reduced bone loss in postmenopausal women: Japanese Population-Based Osteoporosis (JPOS) Study.". The Journal of nutrition 136 (5): 1323–8. PMID 16614424.
- ↑ Katsuyama; Ideguchi, S; Fukunaga, M; Saijoh, K; Sunami, S (2002). "Usual dietary intake of fermented soybeans (Natto) is associated with bone mineral density in premenopausal women.". Journal of nutritional science and vitaminology 48 (3): 207–15. PMID 12350079.
- ↑ Sano; Fujita, H; Morita, I; Uematsu, H; Murota, S (1999). "Vitamin K2 (menatetrenone) induces iNOS in bovine vascular smooth muscle cells: no relationship between nitric oxide production and gamma-carboxylation.". Journal of nutritional science and vitaminology 45 (6): 711–23. PMID 10737225.
- ↑ http://www.npicenter.com/anm/templates/newsATemp.aspx?articleid=23259
- ↑ Dam, H. (1935). "The Antihæmorrhagic Vitamin of the Chick.: Occurrence And Chemical Nature". Nature 135 (3417): 652–653. doi:10.1038/135652b0.
- ↑ MacCorquodale, D. W.; Binkley, S. B.; Thayer, S. A.; Doisy, E. A. (1939). "On the constitution of Vitamin K1". Journal of the American Chemical Society 61: 1928–1929. doi:10.1021/ja01876a510.
- ↑ Fieser, L. F. (1939). "Synthesis of Vitamin K1". Journal of the American Chemical Society 61: 3467–3475. doi:10.1021/ja01267a072.
- ↑ Dam, Henrik (December 12, 1946). The discovery of vitamin K, its biological functions and therapeutical application. Nobel Prize lecture
- ↑ Warner, E. D.; Brinkhous, K. M.; Smith, H. P. (1938). Proceedings of the Society of Experimental Biology and Medicine 37: 628.
- ↑ Oldenburg J, Bevans CG, Müller CR, Watzka M (2006). "Vitamin K epoxide reductase complex subunit 1 (VKORC1): the key protein of the vitamin K cycle". Antioxid. Redox Signal. 8 (3-4): 347–53. doi:10.1089/ars.2006.8.347. PMID 16677080.
- ↑ Suttie JW (1985). "Vitamin K-dependent carboxylase". Annu. Rev. Biochem. 54: 459–77. doi:10.1146/annurev.bi.54.070185.002331. PMID 3896125.
- ↑ Presnell SR, Stafford DW (June 2002). "The vitamin K-dependent carboxylase". Thromb. Haemost. 87 (6): 937–46. PMID 12083499.
- ↑ Stafford DW (August 2005). "The vitamin K cycle". J. Thromb. Haemost. 3 (8): 1873–8. doi:10.1111/j.1538-7836.2005.01419.x. PMID 16102054.
- ↑ Whitlon DS, Sadowski JA, Suttie JW (April 1978). "Mechanism of coumarin action: significance of vitamin K epoxide reductase inhibition". Biochemistry 17 (8): 1371–7. doi:10.1021/bi00601a003. PMID 646989.
- ↑ Terlau H, Olivera BM (January 2004). "Conus venoms: a rich source of novel ion channel-targeted peptides". Physiol. Rev. 84 (1): 41–68. doi:10.1152/physrev.00020.2003. PMID 14715910.
- ↑ Buczek O, Bulaj G, Olivera BM (December 2005). "Conotoxins and the posttranslational modification of secreted gene products". Cell. Mol. Life Sci. 62 (24): 3067–79. doi:10.1007/s00018-005-5283-0. PMID 16314929.
- ↑ No Author. http://www.webmd.com/a-to-z-guides/prothrombin-time
- ↑ Thane CW, Bates CJ, Shearer MJ, et al (June 2002). "Plasma phylloquinone (vitamin K1) concentration and its relationship to intake in a national sample of British elderly people". Br. J. Nutr. 87 (6): 615–22. doi:10.1079/BJNBJN2002582. PMID 12067432.
- ↑ McKeown NM, Jacques PF, Gundberg CM, et al (June 2002). "Dietary and nondietary determinants of vitamin K biochemical measures in men and women". J. Nutr. 132 (6): 1329–34. PMID 12042454. http://jn.nutrition.org/cgi/pmidlookup?view=long&pmid=12042454.
- ↑ Yamano M, Yamanaka Y, Yasunaga K, Uchida K (September 1989). "Effect of vitamin K deficiency on urinary gamma-carboxyglutamic acid excretion in rats". Nippon Ketsueki Gakkai Zasshi 52 (6): 1078–86. PMID 2588957.
- ↑ Bentley R, Meganathan R (September 1982). "Biosynthesis of vitamin K (menaquinone) in bacteria". Microbiol. Rev. 46 (3): 241–80. PMID 6127606. PMC 281544. http://mmbr.asm.org/cgi/pmidlookup?view=long&pmid=6127606.
- ↑ Haddock BA, Jones CW (March 1977). "Bacterial respiration". Bacteriol Rev 41 (1): 47–99. PMID 140652. PMC 413996. http://mmbr.asm.org/cgi/pmidlookup?view=long&pmid=140652.
- ↑ Shearer MJ (January 1995). "Vitamin K". Lancet 345 (8944): 229–34. doi:10.1016/S0140-6736(95)90227-9. PMID 7823718.
- ↑ American Academy of Pediatrics Committee on Fetus and Newborn (July 2003). "Controversies concerning vitamin K and the newborn. American Academy of Pediatrics Committee on Fetus and Newborn". Pediatrics 112 (1 Pt 1): 191–2. PMID 12837888. http://pediatrics.aappublications.org/cgi/pmidlookup?view=long&pmid=12837888.
- ↑ "Routine administration of vitamin K to newborns", Journal of Paediatrics and Child Health (1997) 2(6):429–31
- ↑ Drenckhahn, D. & Kugler, P (2003), "Knochengewebe". In Benninhoff & D. Drenhahn, Anatomie Band 1:147. Munich, Germany: Urban & Fisher
- ↑ 45.0 45.1 Dr. Susan E. Brown, PhD. "Key vitamins for bone health — vitamins K1 and K2". womentowomen.com. http://www.womentowomen.com/bonehealth/keynutrients-vitamink.aspx. Retrieved 11 August 2010.
- ↑ 46.0 46.1 Kanai, T (1997). "Serum vitamin K level and bone mineral density in post-menopausal women". International Journal of Gynecology & Obstetrics 56: 25. doi:10.1016/S0020-7292(96)02790-7.
- ↑ Cheung, AM (2008). "Vitamin K supplementation in postmenopausal women with osteopenia (ECKO trial): a randomized controlled trial". PLoS Med. 5 (10): e196. PMID 9925126. http://www.ncbi.nlm.nih.gov/pubmed/18922041?dopt=Abstract.
- ↑ Feskanich, Diane; Weber, P; Willett, W; Rockett, H; Booth, S; Colditz, G (1999). "Vitamin K intake and hip fractures in women: a prospective study". American Journal of Clinical Nutrition 69 (1): 74. PMID 9925126. http://www.ajcn.org/cgi/pmidlookup?view=long&pmid=9925126.
- ↑ Allison (2001). "The possible role of vitamin K deficiency in the pathogenesis of Alzheimer's disease and in augmenting brain damage associated with cardiovascular disease.". Medical hypotheses 57 (2): 151–5. doi:10.1054/mehy.2001.1307. PMID 11461163.
- ↑ "Vitamin K Found to Protect Against Liver Cancer"
- ↑ Saxena SP, Israels ED, Israels LG (2001). "Novel vitamin K-dependent pathways regulating cell survival.". Apoptosis 6 (1-2): 57–68. doi:10.1023/A:1009624111275. PMID 11321042.
- ↑ Nimptsch K, Rohrmann S, Linseisen J (April 2008). "Dietary intake of vitamin K and risk of prostate cancer in the Heidelberg cohort of the European Prospective Investigation into Cancer and Nutrition. (EPIC-Heidelberg)". Am. J. Clin. Nutr. 87 (4): 985–92. PMID 18400723. http://www.ajcn.org/cgi/pmidlookup?view=long&pmid=18400723.
- ↑ Stenflo J, Fernlund P, Egan W, Roepstorff P (July 1974). "Vitamin K dependent modifications of glutamic acid residues in prothrombin". Proc. Natl. Acad. Sci. U.S.A. 71 (7): 2730–3. doi:10.1073/pnas.71.7.2730. PMID 4528109.
- ↑ Nelsestuen GL, Zytkovicz TH, Howard JB (October 1974). "The mode of action of vitamin K. Identification of gamma-carboxyglutamic acid as a component of prothrombin". J. Biol. Chem. 249 (19): 6347–50. PMID 4214105. http://www.jbc.org/cgi/pmidlookup?view=long&pmid=4214105.
- ↑ Magnusson S, Sottrup-Jensen L, Petersen TE, Morris HR, Dell A (August 1974). "Primary structure of the vitamin K-dependent part of prothrombin". FEBS Lett. 44 (2): 189–93. doi:10.1016/0014-5793(74)80723-4. PMID 4472513.
External links
- Jane Higdon, "Vitamin K", Micronutrient Information Center, Linus Pauling Institute
- Vitamin K: Another Reason to Eat Your Greens
- Vitamin K: Signs of Deficiency
- Vitamin K: Vitamin Deficiency, Dependency, and Toxicity: Merck Manual Professional
- An Alternative Perspective on Vitamin K Prophylaxis
- Health Benefits of Vitamin K2
- Vitamin K content: USDA National Nutrient Database for Standard Reference, Release 19
|
||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||
|
||||||||||||||||||||||||||||||